
Most hospital finance teams know agency nursing is expensive. Fewer have done the line-by-line math on what that actually costs versus the alternative.
This post does that math. Broken down by shift, month, and year, with the variables that move the number up or down.
What You Actually Pay an Agency
The headline bill rate is not the full number. Here is what agency travel nursing costs when you account for all of it.
Direct bill rate: $80–$120 per hour for a registered nurse in 2026, depending on specialty, geography, and contract length. ICU and ED nurses sit at the top of that range. Med-surg is lower. Per-diem agency nurses (short-notice fills) often carry a premium above travel rates.
Overtime exposure: Agency contracts typically guarantee a minimum number of hours per week. If census drops and you do not need those hours, you still pay them. Many contracts include cancellation penalties if you cut shifts below the contracted minimum.
Onboarding and orientation time: Most agencies bill from day one of the contract. The first 1–3 shifts of a travel nurse assignment involve orientation, time you are paying bill rate for productivity you are not fully receiving.
Recruiter and agency margin: Embedded in that bill rate is agency margin, typically 25–40% of the total bill. On a $90/hour rate, you are paying $22–$36/hour directly to the agency, not to the nurse.
No conversion pathway: When a travel nurse is a good fit and you want to hire them permanently, most agency contracts charge a conversion fee, typically 15–25% of the nurse's first-year salary. On a $75,000 salary, that is $11,000–$18,000 to hire someone you already trained and trust.
Total cost per 12-hour agency shift at $90/hour: $1,080 per shift. Plus any overtime or cancellation exposure above contracted minimums.
What You Pay With an IRP
An IRP nurse filling the same shift is your employee, or a per-diem worker, paid their direct hourly rate plus an IRP premium.
Base hourly rate: Typically $35–$50/hour for an RN depending on market, experience, and specialty. This is what you are paying without the agency margin embedded in it.
IRP per-diem premium: Most organizations pay a shift differential for IRP shifts, typically $3–$8/hour or a flat shift bonus of $50–$100 per shift. This is the incentive structure that makes IRP staff choose your shifts over agency work.
Technology platform cost: A technology-enabled IRP runs on a platform. DirectShifts charges a platform fee rather than per-placement fees. At scale, the per-shift platform cost is a small fraction of the bill rate difference.
Credentialing and onboarding (one-time per staff member): The upfront cost of credentialing an IRP nurse is a one-time investment that amortizes across every shift that nurse fills. An agency re-credentials every new traveler on every contract.
Total cost per 12-hour IRP shift at $42/hour base + $6/hour premium: $576 per shift, a $504 savings per shift against the same agency bill.
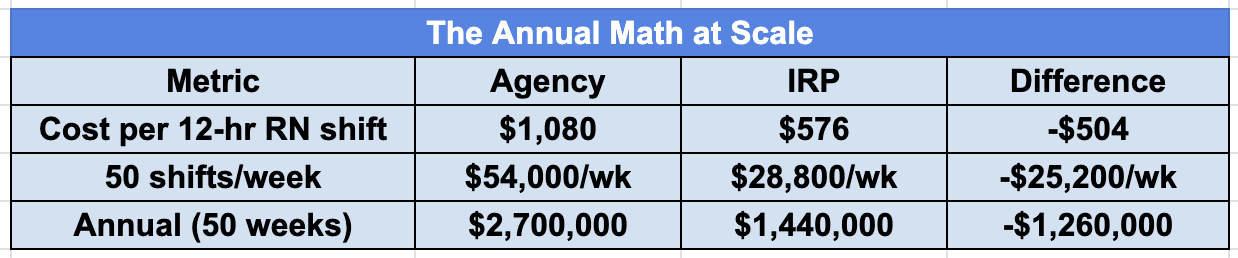
That is a $1.26 million annual difference for a hospital running 50 agency-covered shifts per week, and 50 shifts per week is a modest number for a mid-sized community hospital with regular census variability.
At 100 shifts per week, the annual difference exceeds $2.5 million. That math is why health system CFOs are paying attention to IRP.
The Variables That Change the Outcome
Not every scenario produces the same savings. Here is what moves the number.
Your current bill rates: If you are negotiating lower agency rates than average, say $75/hour, your per-shift savings narrow. If you are paying premium rates for short-notice fills ($110–$130/hour), your savings widen dramatically.
Your IRP nurse mix: A deeper IRP bench means more shifts filled internally. A shallow bench means more fallback to agency. The savings model assumes you can consistently fill the majority of target shifts through the IRP, that requires investing in bench-building early.
Specialty mix: ICU and ED shifts save more per fill than med-surg, simply because the bill rate differential is larger. If most of your agency spend is in high-acuity units, your ROI case is stronger.
Geographic market: Agency rates are higher in California, New York, and major metros. If your facilities are in those markets, your per-shift savings are at the top of the range.
Conversion value: If you are regularly converting travel nurses to permanent staff and paying conversion fees, model that cost separately. IRPs eliminate conversion fees entirely on staff you hire from your own pool.
What the Cost Comparison Misses
Pure cost-per-shift math is the right starting point but it is not the whole picture.
Care continuity: Agency nurses are new to your units, your patients, your protocols. IRP nurses are not. Research consistently shows that continuity of care correlates with better patient outcomes and lower error rates. The value of that continuity does not appear on a staffing cost spreadsheet but it is real and it matters to clinical leadership.
Staff morale: Permanent staff who watch agency nurses earn dramatically more for the same work on the same unit develop resentment that drives turnover. Turnover is expensive, KLAS Research puts the cost of replacing a single RN at $40,000–$60,000 including recruiting, onboarding, and productivity loss. An IRP model that pays your own staff premium rates for extra shifts addresses this dynamic directly.
Budget predictability: Agency costs are unpredictable, they spike with census, with flu season, with resignation waves. IRP costs are more controllable because the rates are set and the pool is managed internally. Finance teams building labor budgets prefer predictable cost structures.
The Transition Timeline
Moving from agency-dependent to IRP-primary does not happen overnight. Realistic timeline for a 200–500 bed facility:
Months 1–3: Platform setup, initial IRP enrollment and credentialing, bench-building. Some shifts begin filling through IRP while agency contracts continue.
Months 4–9: IRP bench reaches functional depth. Agency usage starts declining. Per-shift savings begin materializing.
Months 10–18: IRP covers the majority of flexible staffing needs. Agency is reserved for volume spikes and specialty coverage outside IRP scope.
Year 2+: Fully optimized model. Agency spend reduced by 50–80% depending on organization size and commitment to IRP growth.
The organizations that reach year-two savings fastest are the ones that invest in bench-building in months 1–3, rather than waiting for the IRP to fill itself.
Frequently Asked Questions
How much does a travel nurse actually cost a hospital per hour?The total agency bill rate for a travel nurse in 2026 runs $80-$120 per hour depending on specialty, location, and contract length. ICU and ED nurses are at the top of that range. Med-surg is lower. Short-notice per-diem fills through agencies often carry a premium above travel rates. Embedded in that bill rate is agency margin of 25-40%, meaning $22-$36 of every hour billed goes directly to the agency, not the nurse.
How much cheaper is an IRP nurse compared to a travel nurse?An IRP nurse filling the same shift typically costs $45-$65 per hour, including a per-diem premium to incentivize shift pickup. Against a $90/hour agency bill rate, that is a $25-$45 per hour difference. On a 12-hour shift, the per-shift savings run $300-$540. At 50 shifts per week over a year, the difference exceeds $1 million.
What percentage of a hospital's labor cost should go to agency staffing?The industry benchmark for a well-managed acute care hospital is 3-8% of total labor expense in agency and contract staff. Many hospitals are still running 12-20% post-pandemic and have not brought it down. Above 12% is generally considered a structural problem rather than a managed strategy.
Do hospitals pay a fee when they want to hire a travel nurse permanently?Yes. Most agency contracts include a conversion fee when a hospital hires a travel nurse into a permanent position, typically 15-25% of the nurse's first-year salary. On a $75,000 salary that is $11,000-$18,000 per hire. For hospitals converting 10-15 travel nurses per year to permanent staff, that is $110,000-$270,000 annually in fees, paid to hire people you already vetted and trained.
Is it worth renegotiating agency rates instead of building an IRP?Renegotiating agency rates typically produces modest reductions, usually $3-7 per hour, without changing the underlying cost structure. The agency margin and the markup model stay intact. An IRP replaces the model entirely rather than trimming the edges of it. For hospitals spending more than $500,000 per year on agency staff, the savings from an IRP are an order of magnitude larger than what rate negotiation typically delivers.
What happens to agency costs when you switch to an IRP?Most organizations do not eliminate agency immediately. The IRP fills what it can, agency covers the rest, and the proportion shifts over 12-18 months as the IRP bench grows. Hospitals that reach full IRP maturity typically reduce agency spend by 50-80% compared to pre-IRP baseline. Agency becomes the exception for true spikes and specialty gaps rather than the default for routine gaps.
Empower Your Healthcare Workforce
Subscribe for industry insights, recruitment trends, and tailored solutions for your organization.
Share:




%20(3).png)

%20(1).png)
%20(2).png)




