
The rules for hiring a nurse practitioner are not national. They are determined by the state your clinic operates in, and the difference between a full practice authority state and a restricted practice state can cost you $10,000 to $30,000 per NP per year before you factor in legal fees, compliance overhead, and the time your operations team spends tracking it all.
This guide covers every supervision tier, what it costs, and the specific requirements your NPs will face in the states where physician oversight is still legally required.
The Three-Tier System: What It Actually Means for Employers
Every state falls into one of three categories. The terminology matters less than what each category requires your organization to do.
Full Practice Authority (FPA): No physician agreement required. The NP can diagnose, treat, prescribe controlled substances, and own or operate a practice without physician oversight. About 30 states and Washington D.C. are here as of mid-2026. Hiring in these states is straightforward from a compliance standpoint.
Reduced Practice: A Collaborative Practice Agreement (CPA) with a physician is required for at least one function, most commonly prescribing controlled substances. The NP can practice independently in other respects. If you hire an NP in a reduced practice state and do not secure a CPA before they start, they cannot legally prescribe. That is not a technicality. It is a license risk and a billing problem.
Restricted Practice: Physician supervision is required for most or all clinical functions. This is not just a prescribing requirement. In many restricted states, the NP cannot independently manage patient care without a physician overseeing the arrangement. These states have the highest compliance burden, the most specific documentation requirements, and the most expensive physician agreements.
Full Practice Authority States (No Physician Agreement Required)
As of April 2026, the following states grant full practice authority with no physician collaboration required:
Alaska, Arizona, Colorado, Connecticut, Delaware, Hawaii, Idaho, Iowa, Maine, Maryland, Massachusetts, Minnesota, Montana, Nebraska, Nevada, New Hampshire, New Mexico, North Dakota, Oregon, Rhode Island, South Dakota, Vermont, Virginia, Washington, and Wyoming, plus Washington D.C.
Important nuances in FPA states:
Several of these states grant FPA only after a required transition period. Connecticut, Virginia, and Delaware each require NPs to complete a defined period of supervised practice before they can practice fully independently. Employers hiring new graduates in these states should verify whether the NP has completed the required transition hours before assuming no physician agreement is needed.
New York (status in flux as of mid-2026): New York's FPA law, passed in 2022, allowed NPs to practice independently after completing a 3,600-hour transition period. That law expires July 1, 2026. If the legislature fails to pass Bill S2360 before that date, thousands of experienced NPs in New York will legally lose independent practice status overnight and will need a collaborating physician to continue seeing patients. Employers with NPs in New York should monitor this closely and have a contingency plan.
Employer cost in FPA states: No mandatory physician supervision cost. However, employers may still choose to provide physician consultation resources as a quality or risk management measure. That is a business decision, not a legal requirement.
Reduced Practice States: What You Pay and What the Agreement Must Cover
In reduced practice states, a Collaborative Practice Agreement is a legal condition of NP prescribing. Below are the states where this applies and what the requirements look like.
Florida
Status: Reduced practice. Physician collaboration required.What the agreement must include: Drugs, devices, and treatments the NP may prescribe; general supervision method; quality assurance protocols; and emergency escalation procedures. Supervision does not require the physician to be on-site, but the degree and method of supervision must be documented in the written protocol.Enforcement note: Wellness clinics, IV therapy, and telehealth operations face higher enforcement scrutiny in Florida. Employers in aesthetic or concierge medicine should pay particular attention to CPA specificity.Typical monthly cost: $700 to $1,200 depending on specialty and prescriptive authority scope.
Georgia
Status: Reduced practice.What the agreement must include: Georgia requires a state-specific CPA form to be completed, signed, and submitted before the NP can legally practice. This is not a retention-only requirement. The agreement must be filed.Typical monthly cost: $600 to $1,000.
Illinois
Status: Reduced practice.Key requirement: A written collaborative agreement is required. NPs must practice within the guidelines established by the agreement for at least one element of practice.Typical monthly cost: $600 to $1,000.
Indiana
Status: Reduced/restricted depending on function.Key requirement: Collaborative agreements required. Prescribing authority tied to the agreement.Typical monthly cost: $500 to $900.
Kansas
Status: Reduced practice.Key requirement: Collaborative agreement required for prescribing. The agreement must be available for review.Typical monthly cost: $500 to $900.
Kentucky
Status: Reduced practice.Key requirement: Collaborative practice agreement required. Prescribing and practice scope defined by the agreement.Typical monthly cost: $600 to $950.
Louisiana
Status: Reduced practice.Key requirement: Collaborative practice agreement required. Louisiana NPs must submit agreements to the board.Typical monthly cost: $600 to $1,000.
Michigan
Status: Reduced practice.Key requirement: Collaborative agreement required for prescribing. Specialty alignment between the NP and collaborating physician is an important consideration for agreement validity.Typical monthly cost: $700 to $1,100.
New Jersey
Status: Reduced practice, actively in flux.What happened: New Jersey's pandemic-era prescribing waivers expired February 16, 2026, reinstating the joint protocol requirement. NPs who had been prescribing without a formal protocol under the waiver must now have a compliant agreement in place. Senate Bill 2996 was introduced in January 2026 to grant permanent FPA to NPs with 2,400 hours of experience, but as of mid-2026 it has not passed.Employer action required: Any NJ employer who assumed pandemic-era flexibility still applied needs to confirm their NPs have compliant joint protocols now.Typical monthly cost: $700 to $1,100.
North Carolina
Status: Reduced practice with layered board approval.What the agreement must include: Prescribing authority, emergency procedures, patient population, and a written quality assurance plan. The CPA must be reviewed and signed annually by both the NP and the physician.Chart review requirements: Monthly for the first six months of the agreement, then quarterly after the initial period.Physician on-site requirement: Not required, but the collaborating physician must remain accessible.Typical monthly cost: $800 to $1,200.
Pennsylvania
Status: Reduced practice.Key requirement: Collaborative agreement required. Pennsylvania has a formal collaborative agreement structure that must be maintained on file.Typical monthly cost: $700 to $1,100.
Tennessee
Status: Reduced practice with some of the most operationally demanding requirements of any state.Chart review: The collaborating physician must review at least 20% of patient charts every 30 days.In-person meetings: The NP and collaborating physician must meet in person at least twice per year to review patient care, discuss practice needs, and evaluate protocols.Physician-to-NP ratios: Specific ratio caps apply.CPA filing: Must be on file and available for inspection. Reviewed annually.Cost implication: Tennessee's 20% monthly chart review requirement means per-chart fee structures can become expensive at scale. Employers running high-volume NP clinics in Tennessee should model this against a flat monthly fee before choosing a compensation structure.Typical monthly cost: $900 to $1,500 depending on patient volume.
Texas
Status: Reduced practice. Delegation model with strict prescriptive authority requirements.What the agreement must include: A Delegated Authority Protocol outlining the NP's scope of practice, plus a supervisory structure document. These are two separate required components.Prescriptive authority: Delegation agreements required for any prescribing privileges. Specific drug class authorization must be documented.Chart review: A portion of charts must be reviewed monthly.Physician-to-NP ratios: Strict ratio caps apply. With Texas being one of the largest NP markets in the country, finding physicians willing to collaborate can take longer than in smaller states.On-site requirements: May be required depending on practice scope.CPA registration: Texas requires only notification of the collaborative relationship rather than formal board submission, but the agreement itself must be comprehensive.Typical monthly cost: $1,000 to $2,000. Rates are higher than most states because ratio caps limit physician supply relative to NP demand.
Restricted Practice States: Highest Compliance Burden, Highest Cost
These states require physician oversight for most or all clinical functions. There is generally no hours-based path to independence. The supervision requirement is career-long.
Alabama
Status: Restricted practice. One of the most documentation-intensive states in the country.Pre-practice filing: Approval required before the NP can see patients. In Alabama, care cannot legally begin until the collaboration is filed and approved by the board.Physician on-site requirement: For NPs with fewer than two years (4,000 hours) of clinical experience, the collaborating physician must be present for at least 10% of the NP's scheduled hours. After crossing the 4,000-hour threshold, the physician must meet with the NP no less than quarterly and visit remote sites at least twice annually.NP-to-physician ratio: Specific ratio caps apply.Chart review: QA required with quarterly meetings.Registration fee: $200 at the time the collaboration is registered with the board.Path to independence: None for most NPs under current Alabama law.Typical monthly cost: $1,000 to $1,800. The on-site requirement for new NPs substantially increases cost because it limits the ability to use remote collaboration agreements.
Arkansas
Status: Restricted practice with a defined experience-based pathway toward independence.Key requirement: Collaborative agreement required. QA documentation required.Typical monthly cost: $700 to $1,100.
Mississippi
Status: Restricted practice. Strict physician oversight expectations and limited flexibility for scaling without expanding physician coverage.Path to independence: None under current law.Typical monthly cost: $800 to $1,200.
Missouri
Status: Restricted practice. Among the most operationally demanding states for employers.Chart review: 10% of all charts must be reviewed every 14 days. For controlled substance prescribing, 20% of those charts must be reviewed every 14 days.Physician-to-NP ratio: A collaborating physician may not enter into arrangements with more than six full-time equivalent APRNs or PAs combined.Geographic proximity: The collaborating physician must be located within 75 miles of the NPs they supervise.On-site requirement: The physician must be on-site for the first month before the NP can practice independently. For controlled substances, in-person supervision is required during this initial period.Filing requirement: Within 30 days of any change, and with each physician license renewal.Cost implication: The 14-day chart review cadence is the most frequent mandatory review requirement of any state. This substantially increases the physician's workload and their monthly fee. For employers running controlled substance programs in Missouri, per-chart costs can run significantly higher than in other states.Typical monthly cost: $1,200 to $2,000. Proximity caps and ratio limits make physician sourcing difficult, especially in rural areas. Missouri has no path to NP independence under current law, and at least one active lawsuit in 2025-2026 is challenging the constitutionality of this framework.
Ohio
Status: Listed as full practice authority by some sources but still requires a Standard Care Arrangement (SCA) for most NPs. Verify directly with the Ohio Board of Nursing for current requirements, as Ohio's classification shifted in recent regulatory updates.Key requirement: Standard Care Arrangement required. Annual chart review and annual meetings with the collaborating physician.Typical monthly cost: $700 to $1,100.
West Virginia
Status: Requires permanent physician collaboration for most NPs.Key requirement: Collaborative agreement required. No clear independence pathway for most.Typical monthly cost: $700 to $1,100.
Wisconsin
Status: Requires ongoing physician collaboration.Key requirement: Collaborative agreement required.Typical monthly cost: $600 to $1,000.
California: The Transition-to-Practice Model
California is in a category of its own. AB 890, passed in 2020, created a two-phase pathway toward NP independence.
Phase 1: After completing 4,600 hours (roughly three years full-time) under a collaborative agreement in a facility with a physician on-site, the NP qualifies for supervised independent practice.
Phase 2: After an additional three years in that setting, the NP can apply for full independent practice certification (the "104 certification"), allowing them to open their own practice or work without a physician on-site.
As of January 1, 2026, the California Board of Registered Nursing began accepting applications for the 104 certification. The first cohort of NPs who completed the full TTP pathway became eligible this year.
What this means for employers:
- Any NP you hire in California who has not completed the 4,600-hour TTP requires a collaboration agreement
- That agreement must now account for the 2026 MSO mandate: business managers and investors cannot set patient volume quotas, dictate work schedules, or interfere in the clinical relationship between the NP and collaborating physician
- The collaborating physician cannot supervise more than four NPs at any given time under California law (B&P Code § 2836.1)
- For NPs in the TTP phase, employers must maintain attestation records documenting hours toward the 4,600-hour threshold
Typical monthly cost in California: $1,200 to $2,500. Physician-to-NP ratio caps of four NPs per physician create genuine supply constraints in a state with a large NP workforce. Rates are among the highest in the country.
Cost Reference by State Tier
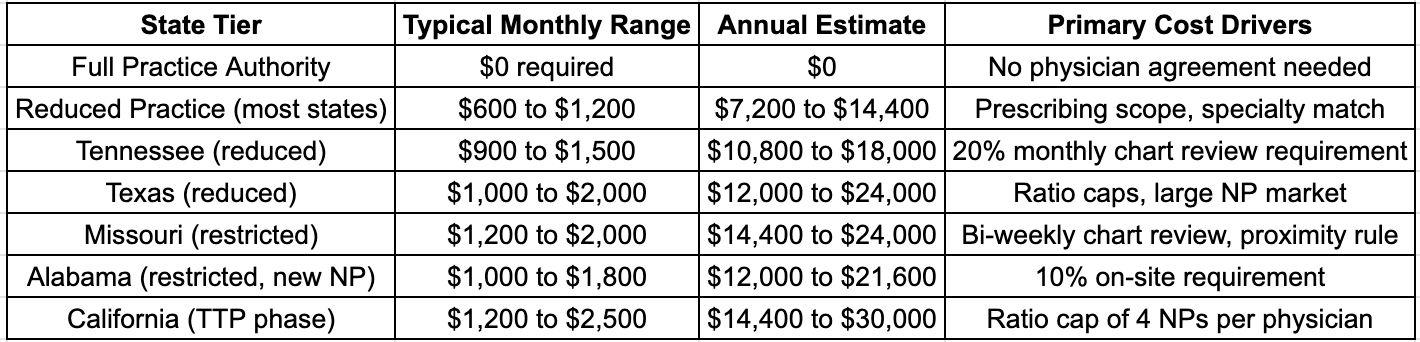
These figures cover the physician fee only. Add $500 to $2,000 for legal drafting of the CPA, recurring annual review costs in states that require re-execution, and internal compliance overhead if you track multiple NPs across sites.
Frequently Asked Questions
Do I need a separate collaborating physician agreement for each NP I hire?
Yes. In states that require physician oversight, the agreement is specific to the NP-physician relationship and the practice setting. If the same physician collaborates with three of your NPs, you typically need three separate agreements, though some states allow omnibus arrangements. Verify the specific requirement for your state.
What happens if my collaborating physician leaves or retires?
The NP cannot practice (or cannot prescribe, in reduced practice states) until a replacement agreement is in place. This is an operational risk most employers underestimate. In states with ratio caps like California, Texas, and Missouri, finding a replacement can take weeks. Build a contingency plan before you need one.
Can a collaborating physician be in a different state?
Some states allow remote or out-of-state collaborating physicians; others require the physician to hold an in-state license and practice within the state. Missouri mandates geographic proximity of 75 miles. Alabama's on-site requirements make remote collaboration difficult for new NPs. Always confirm state-specific proximity requirements before executing an agreement.
Does the collaborating physician need to be the same specialty as the NP?
Not always, but specialty mismatch can be a liability issue and affects the physician's risk exposure and therefore their fee. An internist collaborating with a psychiatric NP may charge more than one working with a primary care NP because their malpractice exposure is outside their core practice area. Some states have specialty alignment guidance; most do not have a hard requirement.
Is a revenue-sharing arrangement with a collaborating physician legal?
It is in most states, but healthcare attorneys generally advise against it. Revenue-based arrangements can raise Stark Law and anti-kickback concerns depending on how the relationship is structured. Flat monthly fees or per-chart fees are the more common and legally cleaner structures.
How do I find a collaborating physician in a restricted practice state?
Physician collaboration platforms, state NP associations, local medical society networks, and healthcare staffing platforms are the primary channels. In high-restriction states with ratio caps, expect a four-to-eight-week sourcing timeline. Hiring NPs before the collaboration agreement is in place creates license risk and billing delays.
Is the collaborating physician liable if my NP makes a clinical error?
In supervisory models, yes, the collaborating physician carries real liability exposure. This is why physicians in restricted states charge more and why high-risk service lines (addiction treatment, mental health with controlled substance prescribing, aesthetics) attract higher collaboration fees.
What Multi-State Employers Need to Know
If you operate NP clinics or employ NPs across multiple states, compliance is not a single-state problem. An NP who is fully independent in Arizona is not automatically independent in Tennessee. Their prescribing authority in Oregon does not extend to Ohio.
Multi-state employers need a state-by-state compliance map for every NP on staff, tracking: the practice authority tier, CPA filing status, physician-to-NP ratio utilization, chart review deadlines, and agreement renewal dates.
Manual tracking across a spreadsheet creates compliance gaps. At scale, the risk is not hypothetical. A single lapsed agreement in a restricted state can trigger a board inquiry, create billing liability if claims were submitted during the lapse period, and put the NP's license at risk.
The states most likely to create compliance problems for multi-site employers are the ones with the most specific documentation requirements: Missouri (bi-weekly chart review), Tennessee (monthly 20% review plus in-person meetings), Alabama (on-site requirements and board registration), and California (TTP hour tracking and annual attestation records).
The Bottom Line
If you hire NPs in restricted or reduced practice states, physician supervision is a line item in your operating model, not an afterthought. The cost ranges from manageable to significant depending on the state. What makes it expensive is not just the monthly fee. It is the legal drafting, the compliance tracking, the sourcing lead time, and the operational risk if the collaboration breaks down.
The employers who handle this well treat it the same way they treat credentialing or malpractice coverage: as infrastructure, not paperwork. Know which states your NPs are in, what those states require, and what it actually costs. Build that into your budget before the hire, not after.
DirectShifts is an AI-powered healthcare staffing platform that helps clinics and health systems hire nurse practitioners and other advanced practice providers. For NP hiring support, including physician collaboration sourcing in restricted and reduced practice states, visit directshifts.com.
Optimize your healthcare operations with advanced solutions that enhance efficiency and improve patient care. Discover strategies to streamline processes and boost productivity.
Schedule a DemoEmpower Your Healthcare Workforce
Subscribe for industry insights, recruitment trends, and tailored solutions for your organization.
Share:




%20(38).png)

%20(15).png)
%20(17).png)




